
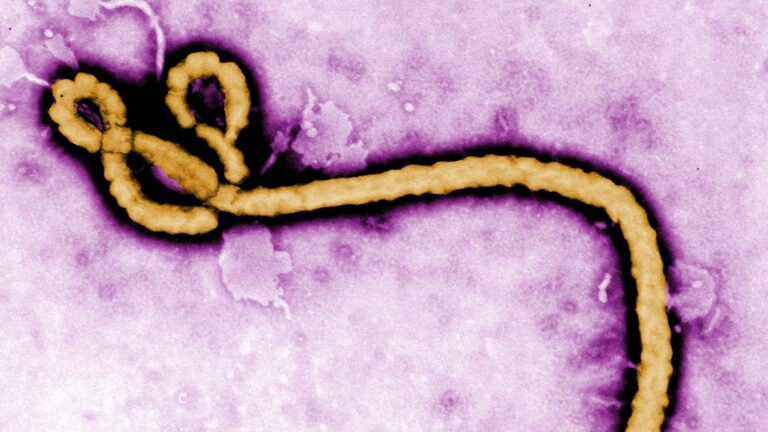
Colorized transmission electron micrograph of an Ebola virus virion. (Photo/Frederick A. Murphy via the Centers for Disease Control and Prevention)
Worried about Ebola? USC virologist has other concerns
Here’s a hint: You might want to think about a flu vaccine
While Ebola continues its march across West Africa and the World Health Organization warns that 20,000 people could be infected in the next six months, USC virologist Paula Cannon is worried about a different disease — the flu.
“Influenza is what keeps me awake — that’s my nightmare scenario,” said Cannon, an associate professor of microbiology at the Keck School of Medicine of USC, where she leads a research team that studies viruses, stem cells and gene therapy.
Globally, Ebola poses less risk than airborne viruses like influenza, which is more contagious and kills as many as 500,000 people annually worldwide, she explained.
Viruses get inside a cell and hijack it.
Paula Cannon
Viruses in general are hard to stop and treat because they’re too much like the humans they invade. “Bacteria are an alien life form and easier to target,” Cannon said. “But viruses get inside a cell and hijack it.” The trick becomes finding what’s unique about the virus, so the treatment destroys it and not the human cell, too.
While Cannon’s primary focus is HIV, she also studies other hemorrhagic fever viruses that cause diseases similar to Ebola, such the rodent-borne arenaviruses Lassa fever and Junin virus. Like Ebola, these distant cousins are RNA viruses, unstable by nature. “Their lifestyle is to act as a swarm, tolerate mutations and adapt to challenges such as drugs that try to target them,” Cannon said.
Strategies tried against other viruses — an HIV-style drug cocktail or antivirals that interfere with viral replication — might work with Ebola, which “doesn’t seem to be a particularly sophisticated viral target,” she noted. However, there are two key obstacles: the lack of financial incentive for pharmaceutical companies to develop vaccine or drugs, and a shortage of the necessary specialized research facilities.
The average drug now costs more than $4 billion to bring to market. That means research into diseases affecting a relative few gets left behind. Plus, Ebola must be studied in a Level 4 Biosafety Laboratory, only a handful of which exist in the U.S.
ZMapp, a combination of three monoclonal antibodies that bind to Ebola, has been used experimentally on a few patients, and it stopped the virus in animal trials. A clinical trial in humans may be fast-tracked to start in 2015. Meanwhile, some researchers are pursuing a faster, cheaper route, trying to identify existing drugs that may have an impact. So far, statins — initially developed to treat heart disease and diabetes — have shown potential against Ebola, as has a drug developed against influenza.
Cannon doesn’t see a major Ebola outbreak happening in the U.S., with its strong medical infrastructure, something lacking in West African countries. She rates the odds “quite likely” that a treatment or vaccine will be developed soon, given the increased interest from this major outbreak. For now, she’s also concerned that climate change might spur new strains of mosquitos to migrate from the tropics to the U.S. That could bring other diseases like dengue fever — and more sleepless nights.


